Service inquiry appointment
WhatsApp:+852 6673 5099
Phone:+852 5801 1515










Keyword search

Family Health Butler
Home »New Health Knowledge »Family Health Butler »Which sinusitis patients are suitable to use this year's popular biologics? |Professor Shi Jianbo's Rhinology Series Science Popularization
Which sinusitis patients are suitable to use this year's popular biologics? |Professor Shi Jianbo's Rhinology Series Science Popularization

In recent years, there has been an increasing amount of literature on the use of biologics for the treatment of type 2 chronic sinusitis with nasal polyps (CRSwNP), and a correct understanding of the relevant issues of biologics in the diagnosis and treatment of the disease has become a problem that every rhinologist must face. Now provide an overview of the relevant issues.
Therapeutic target
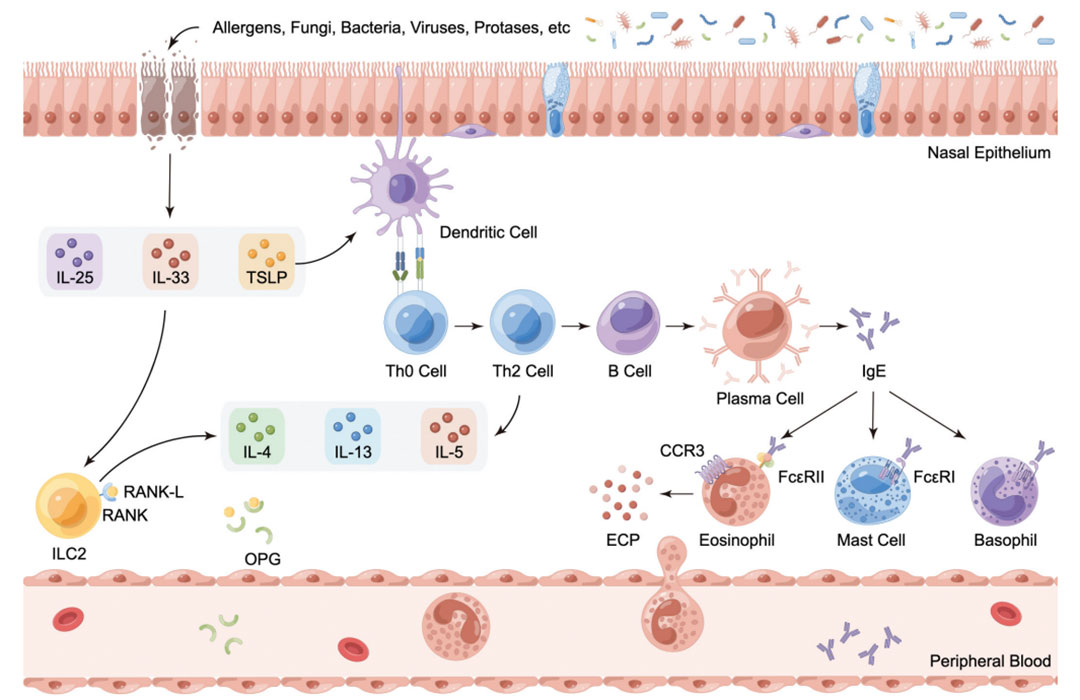
Icon. The main cells and molecules involved in the pathophysiological mechanism of type 2 inflammatory chronic sinusitis with nasal polyps (CRSwNP) have the potential to guide biological therapy as biomarkers. Abbreviation description: CCR3:C-C Motif chemokine acceptor 3; CRSwNP: Chronic sinusitis with nasal polyps; ECP: Eosinophilic cationic protein; IgE: immunoglobulin E;IL: Interleukin; ILC2: Group 2 innate lymphoid cells; OPG: Osteoprotegerin; RANK: nuclear factor κB Acceptor activation factor; RANK-L: nuclear factor κB Acceptor activation factor ligand; Th: auxiliary T Cells; TSLP: Thymic stromal lymphopoietin.
quote Zeyi Jin, Bing Yan, Luo Zhang & Chengshuo Wang (2025) Biological therapy in chronic rhinosinusitis with nasal polyps, Expert Review of Clinical Immunology, 21:4, 473-492, DOI: 10.1080/1744666X.2025.2459929
Currently available types of monoclonal antibodies
1. Resistance IL-4Rα class
(1) Dupilumab: Anti - IL-4 acceptor α A fully human monoclonal antibody (IgG4 type) against the subunit, inhibiting IL-4/IL-13 Signal transduction inhibits type 2 inflammatory pathways.
*At present, the approved indications for Dupilumab in mainland China are not included CRSwNP, Our hospital has completed the registration of super indication drugs for treatment CRSwNP, can be CRSwNP The patient provides the medication
*At present, the approved indications for Dupilumab (Dabitol) in mainland China are not included CRSwNP, Our hospital has completed the registration of super indication drugs for treatment CRSwNP, can be CRSwNP The patient provides the medication
(2) Stapokibart: a domestically produced biological agent, with the same principle as above.
*Our hospital currently also offers Sipuximab (Kangyueda) as a treatment option

2. Resistance IL-5 class
(1) Mepolizumab: anti - IL-5 Humanized monoclonal antibodies can be used with IL-5 Combine and prevent it from binding with the acceptor. Reduce the recruitment, activation, and growth of eosinophils.
(2) Reslizumab: Anti IL-5 Humanized antibodies (intravenous preparations, not yet marketed domestically);
(3) Benralizumab: Targeting IL-5Rα, Mediate eosinophil apoptosis.
3. Resistance IgE
Omalizumab: Anti IgE Humanized monoclonal antibodies can interact with IgE Combining, organizing IgE Reduce the cycle when entering into a contract with the main party IgE Leveling down the activation of mast cells and eosinophils, and reducing local inflammation IgE Driven inflammation.
4. In research/about to be launched
(1) Tezepelumab: a humanized monoclonal antibody against thymic stromal lymphopoietin (TSLP), produced by blocking TSLP Binding with its acceptor, thereby reducing eosinophils IgE、IL-5、IL-13 The generation.
(2) Depemokimab: Ultra Long Acting Antibody IL-5 Monoclonal antibodies with enhanced properties IL-5 Combined with affinity, administer once every six months.
(3) Lebrikizumab: Targeted IL-13 Inhibitors, by binding IL-13, Effectively prevent IL-13Rα1/IL-4Rα The formation of heterodimer complexes blocks subsequent signal transduction.
(4) Tralokinumab: anti - IL-13 Humanization IgG4 Monoclonal antibodies that block their interaction with IL-13 Binding of acceptors (Phase III completed, not yet approved) CRS)。
(5) Itepekimab: a humanized monoclonal antibody against interleukin-33 (IL-33), produced by blocking IL-33/ST2 Signal channels, blocking downstream inflammatory signaling channels (currently) III In progress).
Regarding the indications and timing of medication use
The 2023 European Position paper on Rhinosinusitis and Nasal Polyps (EPOS)/European Forum for Research and Education in Allergy and Respiratory Diseases (EUFOREA) guidelines state that for patients who have undergone endoscopic sinus surgery but still have bilateral nasal polyps CRSwNP patient,If any three of the following five criteria are met simultaneously, the use of biologics for treatment can be considered:
1. There is evidence of type 2 inflammation [blood eosinophil cells (BEC) ≥ 0.15 × 10 ⁹]/ L or IgE≥100IU/mL Or organize ≥ 10 eosinophils/ HPF]。
Regarding Blood Eos≥0.15 ×10⁹/ L As a type 2 inflammation marker, We have different opinions, believing that this value is too low and already lower than the normal population blood Eos The average value is worth discussing
2. Oral hormone therapy ≥ 2 courses/year or long-term (≥ 3 months) low-dose hormone therapy
3. Significant impairment in quality of life [nasal and sinus outcome test (SNOT-22) ≥ 40]
4. Significant loss of sense of smell (olfactory test indicates loss of sense of smell);
5. Combined asthma (requiring regular inhaled hormone therapy).
But if the following situations occur, we believe that priority can be given to using biologics for treatment:
1. Being too old and having poor physical fitness;
2. High disease severity: patients with serious cardiovascular and cerebrovascular diseases, poor control of hypertension and diabetes, high dependence on oral anticoagulants and other basic diseases;
3. Poor response to traditional treatment: For patients with refractory and severe chronic sinusitis accompanied by nasal polyps who have poor therapeutic effects of glucocorticoids and surgical treatment;
4. Patients with poor psychological resilience or psychogenic disorders who are unwilling to accept surgical risks or have no intention of undergoing surgery;
5. Existence of comorbidities: combined with asthma and requiring regular inhalation of glucocorticoids; Oral corticosteroids should be taken for at least 2 courses per year, or there may be contraindications for systemic corticosteroids;
6. Patients with bilateral nasal polyps who still experience disease recurrence after multiple standardized sinus surgeries;
7. Some patients with high risk of recurrence (such as those with surgical contraindications, polyps, and high inflammatory burden) may consider using biologics before and after surgery to improve surgical outcomes and reduce recurrence rates;
8. High net worth individuals.
Evaluation of the therapeutic effect of biologics therapy
1. Evaluation time: Efficacy evaluation should be conducted at 6 months and 12 months.
2. The efficacy is determined based on five specific criteria, including:
(1) Nasal polyp volume reduction ≥ 1 point;
(2) Reduced frequency of oral hormone use or surgical need;
(3) Improvement in quality of life (SNOT-22<40 and improvement exceeding minimal clinically important difference (MCID));
(4) Improvement in smell (through semi objective olfactory testing);
(5) Improvement in comorbidity control (achieved through specific comorbidity scores) MCID)。
If 4-5 criteria are met, it is considered a "superior response", 2-3 criteria are considered a "moderate response", and 0-1 criteria are considered an "ineffective response". If the therapeutic effect is poor, the diagnosis and treatable features need to be re evaluated, and consideration should be given to replacing the biological agent or performing salvage surgery.
Current research and evaluation of biologics
1. Dupilumab
Dupilumab is one of the most comprehensive and significant drugs in current research, especially suitable for refractory conditions CRS Or postoperative recurrence. Dupilumab can significantly reduce nasal polyp scores, improve nasal symptoms (including nasal congestion and reduced sense of smell), and control asthma levels, with efficacy lasting for up to 24 weeks and efficacy data up to two years.
It maintains stable control over the volume of nasal polyps and can maintain therapeutic efficacy regardless of dose reduction (increasing medication intervals). Individualized extended dosing intervals are safe and feasible in most patients, reducing treatment burden while ensuring efficacy. For some patients with unclear early reactions, continuous treatment for more than a year may still result in significant improvement.
2. Sprucubizumab monoclonal antibody
Sprucubizumab in the treatment of severe uncontrolled cases CRSwNP The improvement of nasal polyp volume and nasal congestion symptoms is significantly better than placebo, especially in patients with increased eosinophils.
3. Mabolizumab
Mabolizumab is suitable for patients with postoperative recurrence and eosinophilic inflammation, and has a certain effect in improving nasal congestion and olfaction.
4. Omalizumab
Omalizumab is mainly suitable for patients with poor control of inhaled steroids, which can significantly reduce the use of oral steroids and surgical needs, and the overall efficacy is moderate.
5. Trastuzumab
Tezepril monoclonal antibody as a novel antibody TSLP Biological agents have an early onset time (24 weeks) and a sustained therapeutic effect until 52 weeks, showing significant efficacy in improving nasal symptoms and quality of life. They are effective in treating low BEC(<150 Cell/ μL) With high BEC(>300 Cell/ μL) All patients showed better efficacy than placebo, with the latter having a response amplitude about twice that of the former.
6. Ultra long effect resistance IL-5 Preparation of Demochikumab monoclonal antibody
Demizumab can significantly improve nasal polyp scores and nasal obstruction symptoms by administering twice a year, and has good safety.
Overall, according to literature, resistance TSLP With resistance IL-4Ra Class of drugs have better therapeutic effects than antibiotics IL-5 Class and Resistance IgE Class of drugs, with a 95% confidence interval that does not overlap with other drugs in key clinical studies, suggest their ability to control CRSwNP There may be greater advantages in inflammation and symptom improvement.
In CRSwNP In patients with combined asthma, Dupilumab and Mabolizumab showed dual efficacy, not only improving nasal symptoms, but also helping to control asthma.
Dupilumab is effective against CRSwNP merge NSAID- NSAID aggravated respiratory disease (NERD) patients and non comorbidities NERD The overall therapeutic effect of patients is similar, but they have an advantage in nasal congestion. Mabolizumab is effective in various comorbidities, and nasal polyps are a sign of good response.
Tezepril monoclonal antibody can significantly reduce the frequency of acute exacerbations in asthma patients with nasal polyps, while omalizumab has a relatively stable efficacy in asthma control, regardless of whether it is combined or not CRSwNP influence. BEC The value as a predictive indicator of therapeutic efficacy is becoming increasingly prominent. Research shows that higher baselines BEC Level and treatment with Dupilumab and Mabolizumab SNOT-22 The improvement in ratings is positively correlated. In the study of extending the dosing interval of Dupilumab to 12 weeks, it was found that, BEC Higher frequency patients are more likely to lose disease control during the process of reducing frequency therapy BEC Lower values are more likely to maintain therapeutic efficacy.
From a safety perspective, potential side effects of monoclonal antibodies include:
1. Elevated blood eosinophilia is often a transient reaction, and rare patients may develop eosinophilic granulomatous polyangiitis or eosinophilic pneumonia. It is necessary to be vigilant in identifying and intervening in a timely manner.
2. Joint pain and hyperuricemia.
3. Risk of secondary parasitic infections.
Personalized combination therapy should be adopted for patients based on the intrinsic type of inflammation, comorbidities, and treatment response, including synchronous or sequential use of different biological agents, surgery, immunotherapy, and other methods. In clinical practice, multiple monoclonal antibodies used as perioperative adjuvant therapy can significantly improve nasal congestion and olfactory function, and may be combined with endoscopic sinus surgery (FESS) to improve efficacy.
 click WhatsApp Consultation/Appointment
click WhatsApp Consultation/Appointment
The confusion in clinical treatment
Biological agents are CRSwNP The treatment has opened up new directions, especially showing significant efficacy in patients with refractory or comorbidities. However, in clinical practice, there are still many confusions such as indication selection, treatment course and discontinuation strategy, efficacy evaluation criteria, long-term safety, economic accessibility, and personalized medication, which require more long-term follow-up, real-world research, and prospective clinical trials to solve.
1. Indications and timing of medication
Currently, it is mostly based on severe CRSwNP、 Patients with olfactory dysfunction or asthma, poor response to surgery or corticosteroids, but lacking more precise classification and predictive criteria. There is no consensus on whether it should be used as preoperative assistance, postoperative maintenance, or only for cases of surgical failure or recurrence.
2. Differences in therapeutic efficacy
There are significant individual differences in the efficacy of biologics, and not all patients can benefit. Some patients only show limited efficacy, or even complete ineffectiveness.
3. Treatment duration and discontinuation strategy
Most clinical trials have an observation period of 24-52 weeks, but it is not fully clear whether long-term maintenance is necessary after 1 year of treatment and the risk of recurrence after discontinuation.
4. Safety and tolerability
The overall safety of biologics is good, but there are still risks such as injection reactions, joint pain, and elevated eosinophils. The safety data for long-term use is limited, especially regarding the long-term impact on the immune system.
5. Cost and accessibility
Biological agents are expensive, have a heavy economic burden, and have limited medical insurance coverage. How to strike a balance between cost-effectiveness and patient benefits is a practical dilemma in clinical decision-making.
6. Individualization and lack of biomarkers
Currently, there is a lack of reliable biomarkers to predict therapeutic efficacy and guide personalized medication. EOS, FeNO、IgE、IL-5 Although indicators have certain indicative value, they have not yet become routine clinical tools.